Many women struggle with irregular periods, unexplained fatigue, fertility challenges, mood changes, or low libido without understanding the hormonal cause behind these symptoms. One often-overlooked hormone involved in these issues is prolactin.
Prolactin is produced by the pituitary gland, a small gland located at the base of the brain. Its primary role is supporting breast milk production after childbirth. However, prolactin also influences reproductive hormones, ovulation, immune function, and menstrual regularity.
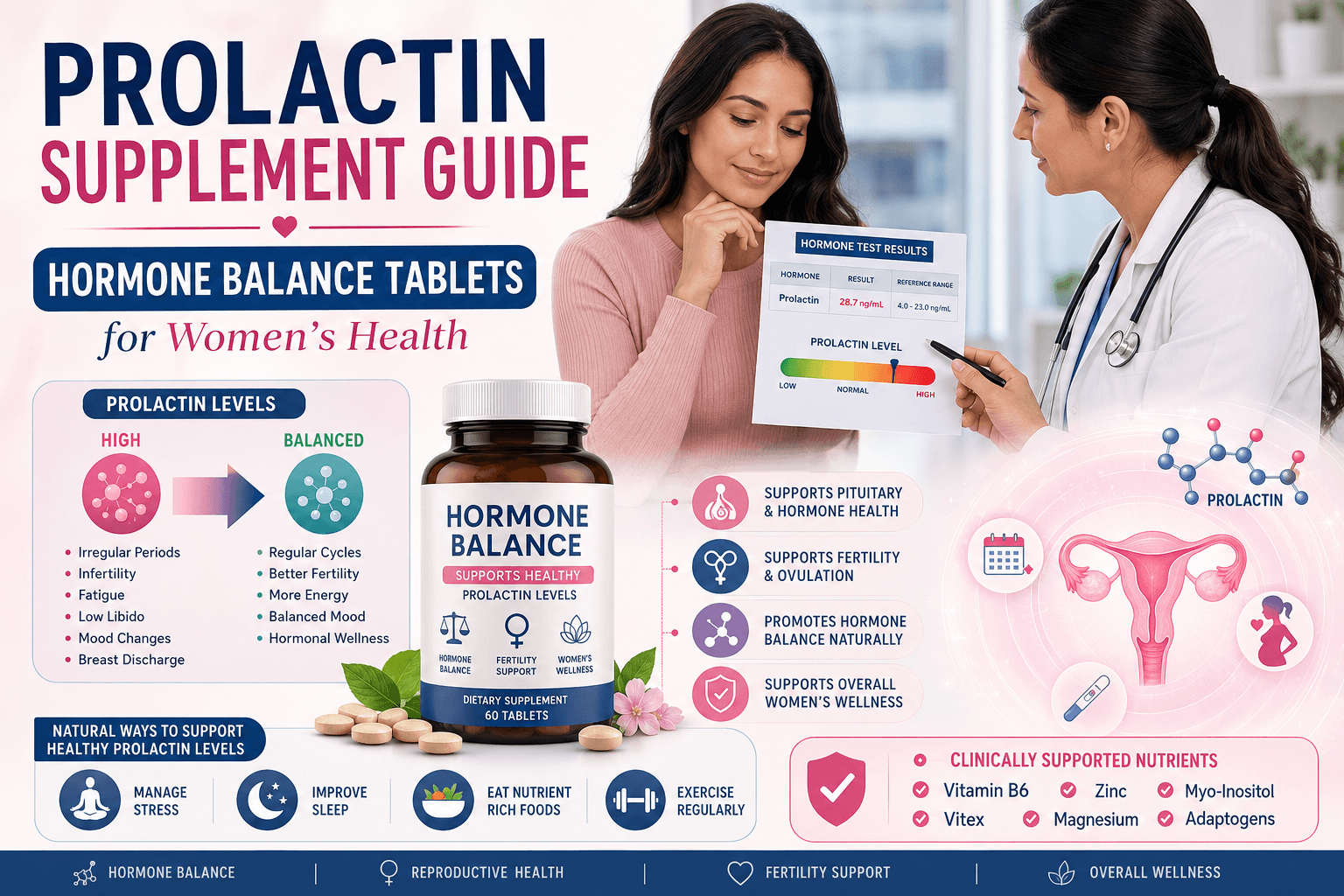
When prolactin levels become abnormally elevated—a condition known as hyperprolactinemia—it can interfere with the hormonal signals responsible for ovulation and healthy menstrual cycles. Understanding this hormone is essential for women experiencing unexplained reproductive health issues, which is why NexGen Health Pakistan provides targeted nutritional support formulated specifically for hormonal balance.
What Happens When Prolactin Levels Rise?
In healthy women, dopamine acts as the body's natural prolactin regulator. Dopamine suppresses prolactin production and keeps hormone levels balanced.
When dopamine levels decline because of stress, nutritional deficiencies, poor sleep, thyroid disorders, or certain medications, prolactin levels may increase.
High prolactin suppresses the release of hormones called LH and FSH, which are essential for ovulation. As a result, women may experience:
Irregular or missed periods
Delayed ovulation
Reduced fertility
Hormonal imbalance
Lower estrogen and progesterone production
This is why prolactin balance is closely linked to menstrual health and conception. Supporting the dopamine pathway through key nutrients like Vitamin B6, zinc, and magnesium—found in quality hormone balance supplements—can help address one of the root causes of elevated prolactin.
Symptoms of High Prolactin
Elevated prolactin often develops gradually. Common symptoms include:
Irregular Menstrual Cycles
One of the earliest signs of high prolactin is a disrupted menstrual cycle. Periods may become infrequent, unpredictable, or stop altogether. Women experiencing persistent cycle irregularities should consider discussing prolactin testing with their healthcare provider and may benefit from supplements like Ovarise Tablet, which supports hormonal balance and menstrual regularity.
Difficulty Conceiving
Since prolactin can suppress ovulation, women may experience fertility challenges despite trying to conceive regularly. Addressing nutritional deficiencies that affect the dopamine-prolactin axis is an important supportive step for women in their preconception journey.
Low Libido and Mood Changes
Reduced estrogen levels can contribute to decreased sexual desire, mood swings, anxiety, and emotional changes. These symptoms often overlap with other hormonal conditions, making proper testing essential.
Breast Discharge
Some women develop galactorrhea, a milky breast discharge unrelated to pregnancy or breastfeeding. This symptom warrants immediate medical evaluation as it may indicate significantly elevated prolactin levels.
Fatigue and Poor Sleep
Hormonal imbalances often affect energy levels, recovery, and sleep quality. Magnesium supplementation may help support better sleep and stress management—key factors in maintaining healthy prolactin levels.
Acne and Hair Changes
Elevated prolactin may contribute to acne breakouts and hair thinning in some women, symptoms that can be mistaken for other hormonal imbalances.
High Prolactin vs PCOS
Many women confuse high prolactin with PCOS because both conditions can cause irregular periods and fertility issues.
PCOS is usually associated with insulin resistance, elevated androgens, and ovarian cysts, whereas hyperprolactinemia primarily involves excessive prolactin production from the pituitary gland.
Because symptoms overlap, proper testing is essential. A hormone panel including prolactin, LH, FSH, testosterone, and thyroid markers can help determine the underlying cause.
Common Causes of Elevated Prolactin
Chronic Stress
Long-term stress increases cortisol production and disrupts dopamine signaling. Lower dopamine allows prolactin levels to rise more easily. Adaptogenic herbs like ashwagandha, combined with magnesium supplementation, can help the body manage stress more effectively and support healthy hormone regulation.
Poor Sleep
Prolactin follows a natural circadian rhythm. Inadequate sleep can disturb hormone regulation and worsen hormonal imbalance. Prioritizing sleep hygiene alongside nutritional support creates a foundation for better hormonal health.
Hypothyroidism
An underactive thyroid is a common cause of elevated prolactin among Pakistani women. In many cases, treating the thyroid issue helps normalize prolactin levels. Women experiencing symptoms of both hypothyroidism and elevated prolactin should request comprehensive thyroid testing (TSH, Free T4) alongside prolactin measurement.
Certain Medications
Some antidepressants, antipsychotics, anti-nausea medications, and blood pressure drugs can increase prolactin levels by affecting dopamine receptors. If you're taking these medications and experiencing hormonal symptoms, discuss them with your doctor before making any changes.
Prolactinoma
A prolactinoma is a non-cancerous pituitary tumor that produces excessive prolactin. This condition requires medical diagnosis and treatment with prescription medications like cabergoline or bromocriptine. Nutritional support is not a substitute for medical treatment in these cases.
Nutritional Deficiencies
Deficiencies in Vitamin B6, magnesium, zinc, and Vitamin B12 can impair dopamine production and contribute to hormonal imbalance. These deficiencies are particularly common among Pakistani women due to dietary patterns and limited sun exposure. Targeted supplementation with products like Sensel SL 2000 MCG (Methylcobalamin B12) can help address these foundational nutritional gaps.
Natural Nutrients That Support Hormone Balance
While supplements are not a replacement for medical treatment, certain nutrients may help support healthy hormone regulation when nutritional deficiencies or lifestyle factors are contributing to mild hormonal imbalance.
Vitamin B6
Vitamin B6 plays a key role in dopamine production. Adequate intake may support the body's natural ability to regulate prolactin levels. Clinical research suggests that B6 supplementation may have modest benefits for women with mild hyperprolactinemia.
Zinc
Zinc supports reproductive hormone function and overall endocrine health. It is commonly found in meat, legumes, and seeds—though many Pakistani diets may be insufficient in this critical mineral.
Magnesium
Magnesium helps regulate stress hormones, improve sleep quality, and support overall hormonal wellness. Since high cortisol is an upstream driver of prolactin elevation, magnesium's stress-buffering properties make it foundational for hormone balance.
Ashwagandha
Ashwagandha is an adaptogenic herb that helps the body manage stress and may indirectly support hormonal balance through cortisol regulation. By reducing the stress response, ashwagandha addresses one of the key lifestyle drivers of prolactin dysregulation.
Vitamin D
Vitamin D deficiency is extremely common among Pakistani women—despite abundant sunshine—due to indoor lifestyles and conservative dress codes. Adequate levels are associated with reproductive health, menstrual regularity, immune function, and overall endocrine wellness. Testing and correcting Vitamin D deficiency should be a priority for women experiencing hormonal symptoms.
Inositol
Myo-Inositol and D-Chiro Inositol are widely used for PCOS management and may help support ovulation, insulin sensitivity, and hormonal balance. For women with overlapping prolactin and PCOS concerns, Ovarise Tablet provides the 40:1 ratio of Myo-Inositol to D-Chiro Inositol that research suggests is most effective.
Vitamin B12
Methylcobalamin, the active form of Vitamin B12, supports nervous system health and dopamine-related pathways involved in hormone regulation. B12 deficiency is common among women with limited animal protein intake. Sublingual delivery, as found in Sensel SL 2000 MCG, enhances absorption and bypasses digestive barriers.
Hormone Health in Pakistan
Hormonal imbalances often go undiagnosed because symptoms are attributed to stress or lifestyle factors. However, several nutritional deficiencies are especially common among Pakistani women.
Many diets are rich in carbohydrates but relatively low in magnesium, zinc, and Vitamin D. Limited sun exposure, indoor lifestyles, and dietary patterns contribute to widespread Vitamin D deficiency.
Including nutrient-rich foods such as eggs, lentils, leafy greens, sesame seeds, beef, fish, and nuts can help improve nutritional status and support hormone health.
For women who struggle to meet nutritional needs through diet alone—whether due to dietary restrictions, food access, or absorption issues—quality supplements from NexGen Health provide a convenient and evidence-based way to address these gaps. All products are available nationwide with cash on delivery, removing barriers for women across Pakistan.
Foods That Support Hormonal Wellness
A balanced diet remains the foundation of hormonal health.
Good dietary sources include:
Eggs for Vitamin D and B12
Lentils and chickpeas (masoor daal, chana daal) for B vitamins and plant protein
Beef and mutton for zinc, B12, and iron
Sesame seeds (til) for magnesium and calcium
Leafy greens (palak, methi) for folate and minerals
Fatty fish for omega-3 fatty acids
Kalonji (nigella seeds) for zinc and anti-inflammatory compounds
No single food can dramatically lower prolactin, but overall nutritional quality influences hormone balance and reproductive health. Combining a nutrient-dense diet with targeted supplementation creates the strongest foundation for hormonal wellness.
Hormone Balance Supplements vs Medical Treatment
The best approach depends on the severity and cause of prolactin elevation.
Hormone balance supplements from NexGen Health may be appropriate for women dealing with nutritional deficiencies, stress-related hormone disruption, or mild hormonal imbalances. They work best as part of a comprehensive approach that includes diet, sleep, and stress management.
Lifestyle improvements—including better sleep, stress management, regular physical activity, and balanced nutrition—should be part of every hormone support plan. These are non-negotiable foundations that no supplement can replace.
However, women with significantly elevated prolactin levels, pituitary tumors, persistent infertility, or absent periods should seek medical evaluation. Prescription medications such as cabergoline or bromocriptine may be necessary when clinically indicated.
High Prolactin and Fertility
Prolactin directly affects fertility because it suppresses the hormones responsible for ovulation—namely LH and FSH.
Without ovulation, natural conception becomes difficult or impossible. Even mild prolactin elevations can affect the luteal phase (the post-ovulation phase governed by progesterone) and reduce the chances of successful implantation.
Women trying to conceive should discuss the following tests with their healthcare provider:
Serum prolactin
Thyroid function tests (TSH, Free T4)
LH and FSH levels
Testosterone and androgen markers
Fasting insulin (if PCOS is suspected)
These tests help identify the root cause of fertility challenges and guide treatment decisions.
When Should You See a Doctor?
Seek medical advice if you experience:
Irregular periods lasting longer than three months
Breast discharge (galactorrhea) unrelated to breastfeeding
Persistent fatigue unresponsive to rest
Severe hormonal symptoms affecting quality of life
Repeated cycle irregularities with no clear cause
A simple blood test can often identify whether elevated prolactin is contributing to your symptoms. Don't delay seeking medical evaluation for persistent symptoms—early diagnosis improves treatment outcomes.
Products That Support Hormonal Balance in Pakistan
NexGen Health Pakistan offers a range of evidence-based supplements formulated to address the nutritional and hormonal needs of Pakistani women:
Contains Myo-Inositol and D-Chiro Inositol in the research-backed 40:1 ratio. Supports ovulation, insulin sensitivity, menstrual regularity, and hormonal balance—particularly beneficial for women with PCOS or irregular cycles.
Sublingual Methylcobalamin (active Vitamin B12) for superior absorption. Supports the dopamine pathway, nervous system function, energy production, and hormonal wellness.
Combines Iron Bisglycinate (gentle, highly absorbable iron), L-Methylfolate (active folate), and Vitamin C. Essential for preconception health, menstrual wellness, and addressing iron deficiency anemia.
Prolactin may not receive the same attention as estrogen or progesterone, but it plays a crucial role in female reproductive health. Elevated prolactin can affect ovulation, menstrual cycles, fertility, mood, and overall wellbeing.
For many women in Pakistan, addressing nutritional deficiencies, improving sleep quality, managing stress, and using evidence-based hormone balance supplements from NexGen Health may help support healthier hormone function. At the same time, persistent symptoms should always be evaluated by a qualified healthcare professional.
Understanding prolactin is the first step toward restoring hormonal balance and making informed decisions about your reproductive health.